Some toddlers walk with a duck-footed gait as they learn to use their new-found ability to walk — it’s also known as out-toeing. This means that they waddle-walk with their toes pointed outward rather than forward.
Out-toeing can also sometimes manifest for the first time in adolescents, teens, or adults. It’s not always a cause of concern, but it’s worth knowing the difference between a natural duck-footed gait and a condition that impacts how you walk.
Read on to learn the causes of this condition, when you should seek health care help, and information about solutions.

What does being duck-footed mean?
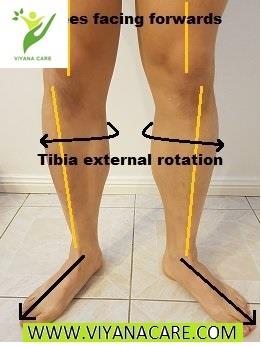
Out-toeing is a type of torsional deformity. It typically occurs when one of the leg’s two longest bones turn toward the outside of the leg, causing the foot to jut out:
tibia: located between the knee and ankle
femur: located between the hip and knee
Out-toeing can occur in one or both legs. In many young children, out-toeing is typically temporary and short-lived. But duck-footedness can persist into adolescence or beyond, sometimes well into adulthood.
Having flat feet can also cause the appearance of out-toeing.
Is it similar to being pigeon-toed?
You may be familiar with a more common torsional deformity called in-toeing — being pigeon-toed. It’s essentially the opposite of being duck-footed.
With a pigeon-toed gait, you walk with your toes pointed in an inward direction rather than outward.
What are the symptoms of being duck-footed?
Out-toeing can make a child look like they’re waddling from side to side. You may notice that your child’s knees also appear to point outward.
Out-toeing is not typically associated with pain or discomfort. It also doesn’t usually interfere with a child’s ability to walk, run, or be mobile in any way.
Out-toeing may be more obvious when a child runs than when they walk. Parents may also notice that their child’s shoes wear out or have more noticeable scuff marks on the outer edges of the shoes.
You can check for out-toeing in adults by standing naturally with your feet about 1 foot apart. Look down at the position of your toes — if they point outward instead of straight ahead, you are probably duck-footed.
Here’s another way to see if you’re duck-footed:
Lie down on your back.
Do your feet turn outward along with your knees? You may have out-toeing caused by tight hip muscles.
What are the causes of being duck-footed?
There are several common causes of out-toeing in toddlers or children, including:
family history of being duck-footed
fetal position of the legs in the uterus prior to birth
resting position of the legs during infancy
being flat-footed
Some rare causes of out-toeing include:
congenital bone deformity
slipped capital femoral epiphysis, a hip condition that causes the ball at the top of the femur to slip backwards.
Slipped capital femoral epiphysis
Capital femoral epiphysis occurs in adolescents or teens who are still growing. It is sometimes referred to as a disorder of the hip growth plate.
In adults, out-toeing may be the result of:
injury to the leg, hip, ankle, or foot
muscle tightness in the legs or hips
poor posture
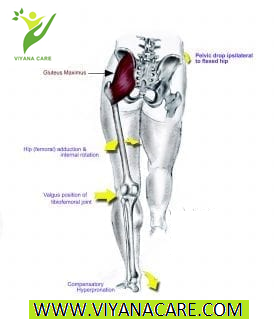
a sedentary lifestyle that results in an anterior pelvic tilt or a pelvis that tips forward
Anterior pelvic tilt in adults
An anterior pelvic tilt causes the hip muscles to tighten, which rotates the femur outward and can result in duck-footedness.
Should I be concerned?
In adults, out-toeing may be mild or extreme. If your condition doesn’t stop you from participating in activities such as walking, running, or swimming, it is not cause for alarm.
If you are concerned about your child’s gait at any point during their development, talk to their doctor.
Children typically outgrow duck-footedness between the ages of 6 and 8. Here are some tips for when you should see a doctor if your child’s condition persists beyond that time or if you’re experiencing symptoms:
Your child limps or falls often while walking or running.
Your child has ongoing or intermittent pain in the legs, hips, or groin — this may indicate slipped capital femoral epiphysis. Pain can be mild or severe, and may be ongoing or come on suddenly.
Your child has a sudden inability to walk (this may also indicate slipped capital femoral epiphysis).
Your condition is severe and causes pain, imbalance, or instability.
Are there home remedies for duck-footedness?
Mild out-toeing can often be resolved with at-home treatment. Here are some remedies you can try at home.
When should I see my doctor?
Any feeling of pain, discomfort, or a lack of mobility should prompt a call to the doctor for both children and adults. You should also contact your child’s doctor if they fall or limp often.
You may also consider seeing a doctor or physical expert before trying to treat mild out-toeing at home.
A professional can determine if your condition is caused by muscle tightness or an outwardly turned tibia or femur. This can help determine what exercises may be most effective.
How is duck-footedness diagnosed?
Here are some of the methods and tests your doctor may use to determine whether you or your child is duck-footed:
Intake: may determine how long the condition has persisted and if there are any incidents that may be the cause. They will also ask about family history.
Physical examination: centers on the legs, hips, and feet. Your doctor will be looking for signs of tightness, lack of flexibility, and range of motion.
Degree of rotation: determined in the leg bones by assessing the angles between the feet and legs. This is typically done by having you lie down on your stomach with knees bent for visual analysis.
Footwear: your health expert may also examine your footwear and have you walk around in your common footwear to see your typical gait.
Running: your health expert may have you run to see if you waddle from side to side as well as examine the position of the feet while in motion.
Imaging tests: your doctor may order X-rays or an MRI if they suspect a serious condition like slipped capital femoral epiphysis.
Are there medical treatments for duck-footedness?
Here are some possible medical treatments for duck-footedness that your doctor may recommend:
Watchful waiting: if your child is under 6 years old, their doctor may recommend watching and waiting to see if the condition resolves on its own.
Physical therapy: a physical therapist can help oversee exercises that may retrain the legs and feet or reduce pressure and tightness in the hips.
Surgery: if a bone deformity or slipped capital femoral epiphysis is found, surgery may be recommended.
Are there any possible complications of being duck-footed?
When severe out-toeing is left unchecked, it may eventually cause other conditions, such as:
muscle atrophy in the lower legs and glutes
knee injury
ankle injury
flat feet
foot pain
damage to the piriformis muscle, which can result in sciatica
The takeaway
Out-toeing, or being duck-footed, is a condition marked by feet that point outward instead of straight ahead.
It’s most common in toddlers and young children, who typically outgrow it by age 8. Adults can also become duck-footed as the result of a sedentary lifestyle, poor posture, injury, or other causes.
This condition is rarely serious and typically responds well to treatments at home. Contact our expert if you have any concerns about your child’s gait.
At The viyanacare center, our team of experience, enthusiastic and highly qualified has worked with numerous professional sports athletes and recreational sport lovers. We will be happy to assess your foot , provide advice on useful exercises to adjust anything that sits outside the normal range, and help you with the choice of footwear depending on how, when and where you .
So if you have any questions about duck-footed , please come and see us at The viyanacare site.
Out-toeing can also sometimes manifest for the first time in adolescents, teens, or adults. It’s not always a cause of concern, but it’s worth knowing the difference between a natural duck-footed gait and a condition that impacts how you walk.
Read on to learn the causes of this condition, when you should seek health care help, and information about solutions.
What does being duck-footed mean?
Out-toeing is a type of torsional deformity. It typically occurs when one of the leg’s two longest bones turn toward the outside of the leg, causing the foot to jut out:
tibia: located between the knee and ankle
femur: located between the hip and knee
Out-toeing can occur in one or both legs. In many young children, out-toeing is typically temporary and short-lived. But duck-footedness can persist into adolescence or beyond, sometimes well into adulthood.
Having flat feet can also cause the appearance of out-toeing.
Is it similar to being pigeon-toed?
You may be familiar with a more common torsional deformity called in-toeing — being pigeon-toed. It’s essentially the opposite of being duck-footed.
With a pigeon-toed gait, you walk with your toes pointed in an inward direction rather than outward.
What are the symptoms of being duck-footed?
Out-toeing can make a child look like they’re waddling from side to side. You may notice that your child’s knees also appear to point outward.
Out-toeing is not typically associated with pain or discomfort. It also doesn’t usually interfere with a child’s ability to walk, run, or be mobile in any way.
Out-toeing may be more obvious when a child runs than when they walk. Parents may also notice that their child’s shoes wear out or have more noticeable scuff marks on the outer edges of the shoes.
You can check for out-toeing in adults by standing naturally with your feet about 1 foot apart. Look down at the position of your toes — if they point outward instead of straight ahead, you are probably duck-footed.
Here’s another way to see if you’re duck-footed:
Lie down on your back.
Do your feet turn outward along with your knees? You may have out-toeing caused by tight hip muscles.
What are the causes of being duck-footed?
There are several common causes of out-toeing in toddlers or children, including:
family history of being duck-footed
fetal position of the legs in the uterus prior to birth
resting position of the legs during infancy
being flat-footed
Some rare causes of out-toeing include:
congenital bone deformity
slipped capital femoral epiphysis, a hip condition that causes the ball at the top of the femur to slip backwards.
Slipped capital femoral epiphysis
Capital femoral epiphysis occurs in adolescents or teens who are still growing. It is sometimes referred to as a disorder of the hip growth plate.
In adults, out-toeing may be the result of:
injury to the leg, hip, ankle, or foot
muscle tightness in the legs or hips
poor posture
a sedentary lifestyle that results in an anterior pelvic tilt or a pelvis that tips forward
Anterior pelvic tilt in adults
An anterior pelvic tilt causes the hip muscles to tighten, which rotates the femur outward and can result in duck-footedness.
Should I be concerned?
In adults, out-toeing may be mild or extreme. If your condition doesn’t stop you from participating in activities such as walking, running, or swimming, it is not cause for alarm.
If you are concerned about your child’s gait at any point during their development, talk to their doctor.
Children typically outgrow duck-footedness between the ages of 6 and 8. Here are some tips for when you should see a doctor if your child’s condition persists beyond that time or if you’re experiencing symptoms:
Your child limps or falls often while walking or running.
Your child has ongoing or intermittent pain in the legs, hips, or groin — this may indicate slipped capital femoral epiphysis. Pain can be mild or severe, and may be ongoing or come on suddenly.
Your child has a sudden inability to walk (this may also indicate slipped capital femoral epiphysis).
Your condition is severe and causes pain, imbalance, or instability.
Are there home remedies for duck-footedness?
Mild out-toeing can often be resolved with at-home treatment. Here are some remedies you can try at home.
When should I see my doctor?
Any feeling of pain, discomfort, or a lack of mobility should prompt a call to the doctor for both children and adults. You should also contact your child’s doctor if they fall or limp often.
You may also consider seeing a doctor or physical expert before trying to treat mild out-toeing at home.
A professional can determine if your condition is caused by muscle tightness or an outwardly turned tibia or femur. This can help determine what exercises may be most effective.
How is duck-footedness diagnosed?
Here are some of the methods and tests your doctor may use to determine whether you or your child is duck-footed:
Intake: may determine how long the condition has persisted and if there are any incidents that may be the cause. They will also ask about family history.
Physical examination: centers on the legs, hips, and feet. Your doctor will be looking for signs of tightness, lack of flexibility, and range of motion.
Degree of rotation: determined in the leg bones by assessing the angles between the feet and legs. This is typically done by having you lie down on your stomach with knees bent for visual analysis.
Footwear: your health expert may also examine your footwear and have you walk around in your common footwear to see your typical gait.
Running: your health expert may have you run to see if you waddle from side to side as well as examine the position of the feet while in motion.
Imaging tests: your doctor may order X-rays or an MRI if they suspect a serious condition like slipped capital femoral epiphysis.
Are there medical treatments for duck-footedness?
Here are some possible medical treatments for duck-footedness that your doctor may recommend:
Watchful waiting: if your child is under 6 years old, their doctor may recommend watching and waiting to see if the condition resolves on its own.
Physical therapy: a physical therapist can help oversee exercises that may retrain the legs and feet or reduce pressure and tightness in the hips.
Surgery: if a bone deformity or slipped capital femoral epiphysis is found, surgery may be recommended.
Are there any possible complications of being duck-footed?
When severe out-toeing is left unchecked, it may eventually cause other conditions, such as:
muscle atrophy in the lower legs and glutes
knee injury
ankle injury
flat feet
foot pain
damage to the piriformis muscle, which can result in sciatica
The takeaway
Out-toeing, or being duck-footed, is a condition marked by feet that point outward instead of straight ahead.
It’s most common in toddlers and young children, who typically outgrow it by age 8. Adults can also become duck-footed as the result of a sedentary lifestyle, poor posture, injury, or other causes.
This condition is rarely serious and typically responds well to treatments at home. Contact our expert if you have any concerns about your child’s gait.
At The viyanacare center, our team of experience, enthusiastic and highly qualified has worked with numerous professional sports athletes and recreational sport lovers. We will be happy to assess your foot , provide advice on useful exercises to adjust anything that sits outside the normal range, and help you with the choice of footwear depending on how, when and where you .
So if you have any questions about duck-footed , please come and see us at The viyanacare site.