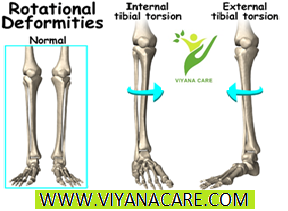
It is a rotation of the lower leg bone (tibia) excessively inwards relative to the upper leg bone (femur). It may also be due to an internal twist of the lower portion of the lower leg bone (tibia) relative to the upper portion of the lower leg bone (tibia). Usually noticed between the ages of 2 and 4. It is the most common cause of intoe in the 2 to 4-year-old age group and the condition usually resolves by age 8.
CAUSE:
Intrauterine position.
Excessive medial ligamentous and muscular tightness around the knee region.
Sitting and sleeping postures (picture below) may perpetuate the problems but generally do not cause them.


SIGNS AND SYMPTOMS:
When viewing the child standing, the foot and lower leg appear to be rotated internally. If there is an isolated problem, the kneecaps appear to be straight, thus distinguishing this condition from femoral anteversion in which the kneecaps are pointed in.
When walking or running the feet excessively turn in occasionally causing tripping and falling. During running the kneecaps continue to stay straight.
At the end of the day when fatigue sets in the intoe appears to be worse. May be asymmetrical (one side worse than the other).
May appear to be bowlegged (because the musculature in the calf is rotated towards the outside of the lower leg).
Could be associated with metatarsus adductus in an infant.

INTERNAL TIBIAL TORSION
It is a rotation of the lower leg bone (tibia) excessively inwards relative to the upper leg bone (femur). It may also be due to an internal twist of the lower portion of the lower leg bone (tibia) relative to the upper portion of the lower leg bone (tibia). Usually noticed between the ages of 2 and 4. It is the most common cause of intoe in the 2 to 4-year-old age group and the condition usually resolves by age 8.
CAUSE:
Intrauterine position.
Excessive medial ligamentous and muscular tightness around the knee region.
Sitting and sleeping postures (picture below) may perpetuate the problems but generally do not cause them.
SIGNS AND SYMPTOMS:
When viewing the child standing, the foot and lower leg appear to be rotated internally. If there is an isolated problem, the kneecaps appear to be straight, thus distinguishing this condition from femoral anteversion in which the kneecaps are pointed in.
When walking or running the feet excessively turn in occasionally causing tripping and falling. During running the kneecaps continue to stay straight.
At the end of the day when fatigue sets in the intoe appears to be worse. May be asymmetrical (one side worse than the other).
May appear to be bowlegged (because the musculature in the calf is rotated towards the outside of the lower leg).
Could be associated with metatarsus adductus in an infant.
CLINICAL EXAMINATION:
Examining the child with the patient sitting, standing and walking is important. When the child is sitting the rotation of the lower leg bone is measured against the upper leg bone. When the rotation of the lower leg bone is excessively in with very little rotation out, this is indicative of internal tibial torsion. Observation of the kneecaps is important in helping to rule out femoral anteversion or to determine if there is a component of a hip problem associated with it.
TREATMENT:
Observation of gait and reassurance to the parents that the condition usually resolves by age 8 is provided.
Abnormal sitting and sleeping postures which tend to perpetuate the deformity need to be changed.
A child that is tripping and falling or has a posture that is excessively turning in will benefit from a cast that goes above the knee. During the cast application the lower leg bone is gently rotated externally relative to the upper leg bone. This helps to stretch the ligamentous and musculotendinous structures around the knee. Cast may be utilized for 2-6 weeks. This will rapidly help the normal physiologic unwinding process of the lower leg bone relative to the upper leg bone.
Night splinting is utilized following cast removal to maintain the correction.
Counter rotational splints and a Denis Browne bar may also be helpful. They may not help as much in the unwinding process as much as they will help prevent abnormal sleeping postures that could perpetuate the deformity.
Orthotics and gait plates may also be utilized to help to move the foot towards external rotation during gait. They are also beneficial in preventing abnormal compensation, which could put stress on the arch.
It is rare that an operation is performed for this condition. If the deformity is excessive causing tripping and falling and there is a significant cosmetic concern, surgery on the lower portion of the lower leg can be performed to externally rotate the foot.
Clinical photograph of an infant with internal tibial torsion. The leg (below the knee) appear deviated internally and slightly rotated internally as well.
The photograph below depicts an adolscent child with the similar type of structural changes with internal deviation of the tibia with interna rotation causing the feet to also turn inward.

How The viyanacare can help you
you will know that your feet need good care all the time, and proper foot healthcare looks at the bigger picture. Your feet are connected to the function of your knees, hips and lower back, and as sport expert we build better bodies from your feet up.
At The viyanacare, our team of experienc , enthusiastic and highly qualified has worked with numerous professional sports athletes and recreational sport lovers. We will be happy to assess your foot rotation, provide advice on useful exercises to adjust anything that sits outside the normal range, and help you with the choice of footwear depending on how, when and where you run.
So if you have any questions about foot rotation, please come and see us at The viyanacare site.
CAUSE:
Intrauterine position.
Excessive medial ligamentous and muscular tightness around the knee region.
Sitting and sleeping postures (picture below) may perpetuate the problems but generally do not cause them.
SIGNS AND SYMPTOMS:
When viewing the child standing, the foot and lower leg appear to be rotated internally. If there is an isolated problem, the kneecaps appear to be straight, thus distinguishing this condition from femoral anteversion in which the kneecaps are pointed in.
When walking or running the feet excessively turn in occasionally causing tripping and falling. During running the kneecaps continue to stay straight.
At the end of the day when fatigue sets in the intoe appears to be worse. May be asymmetrical (one side worse than the other).
May appear to be bowlegged (because the musculature in the calf is rotated towards the outside of the lower leg).
Could be associated with metatarsus adductus in an infant.
INTERNAL TIBIAL TORSION
It is a rotation of the lower leg bone (tibia) excessively inwards relative to the upper leg bone (femur). It may also be due to an internal twist of the lower portion of the lower leg bone (tibia) relative to the upper portion of the lower leg bone (tibia). Usually noticed between the ages of 2 and 4. It is the most common cause of intoe in the 2 to 4-year-old age group and the condition usually resolves by age 8.
CAUSE:
Intrauterine position.
Excessive medial ligamentous and muscular tightness around the knee region.
Sitting and sleeping postures (picture below) may perpetuate the problems but generally do not cause them.
SIGNS AND SYMPTOMS:
When viewing the child standing, the foot and lower leg appear to be rotated internally. If there is an isolated problem, the kneecaps appear to be straight, thus distinguishing this condition from femoral anteversion in which the kneecaps are pointed in.
When walking or running the feet excessively turn in occasionally causing tripping and falling. During running the kneecaps continue to stay straight.
At the end of the day when fatigue sets in the intoe appears to be worse. May be asymmetrical (one side worse than the other).
May appear to be bowlegged (because the musculature in the calf is rotated towards the outside of the lower leg).
Could be associated with metatarsus adductus in an infant.
CLINICAL EXAMINATION:
Examining the child with the patient sitting, standing and walking is important. When the child is sitting the rotation of the lower leg bone is measured against the upper leg bone. When the rotation of the lower leg bone is excessively in with very little rotation out, this is indicative of internal tibial torsion. Observation of the kneecaps is important in helping to rule out femoral anteversion or to determine if there is a component of a hip problem associated with it.
TREATMENT:
Observation of gait and reassurance to the parents that the condition usually resolves by age 8 is provided.
Abnormal sitting and sleeping postures which tend to perpetuate the deformity need to be changed.
A child that is tripping and falling or has a posture that is excessively turning in will benefit from a cast that goes above the knee. During the cast application the lower leg bone is gently rotated externally relative to the upper leg bone. This helps to stretch the ligamentous and musculotendinous structures around the knee. Cast may be utilized for 2-6 weeks. This will rapidly help the normal physiologic unwinding process of the lower leg bone relative to the upper leg bone.
Night splinting is utilized following cast removal to maintain the correction.
Counter rotational splints and a Denis Browne bar may also be helpful. They may not help as much in the unwinding process as much as they will help prevent abnormal sleeping postures that could perpetuate the deformity.
Orthotics and gait plates may also be utilized to help to move the foot towards external rotation during gait. They are also beneficial in preventing abnormal compensation, which could put stress on the arch.
It is rare that an operation is performed for this condition. If the deformity is excessive causing tripping and falling and there is a significant cosmetic concern, surgery on the lower portion of the lower leg can be performed to externally rotate the foot.
Clinical photograph of an infant with internal tibial torsion. The leg (below the knee) appear deviated internally and slightly rotated internally as well.
The photograph below depicts an adolscent child with the similar type of structural changes with internal deviation of the tibia with interna rotation causing the feet to also turn inward.
How The viyanacare can help you
you will know that your feet need good care all the time, and proper foot healthcare looks at the bigger picture. Your feet are connected to the function of your knees, hips and lower back, and as sport expert we build better bodies from your feet up.
At The viyanacare, our team of experienc , enthusiastic and highly qualified has worked with numerous professional sports athletes and recreational sport lovers. We will be happy to assess your foot rotation, provide advice on useful exercises to adjust anything that sits outside the normal range, and help you with the choice of footwear depending on how, when and where you run.
So if you have any questions about foot rotation, please come and see us at The viyanacare site.